What causes tubo-otitis in a child, and how to treat the disease?
Quite often, parents have to deal with such a phenomenon as tubo-otitis in children. Due to the location of inflammation (Eustachian tube) in this disease, it is also called eustachitis or salpingo-otitis. Another name for the pathology, which is widespread among the population far from medicine, is otitis media. The severity of the disease is due to the severity of the inflammatory process, which affects deep structures, severe pain and the likelihood of complications.
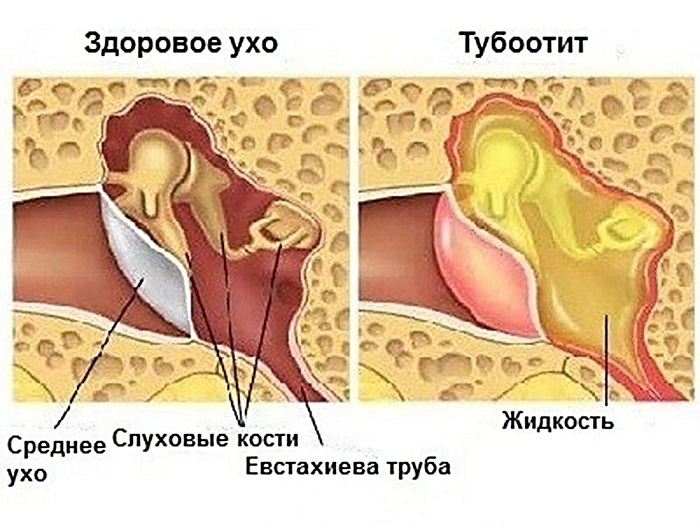
Tubo-otitis is diagnosed when the mucous membrane lining the surface of the auditory (Eustachian) tube and tympanic cavity becomes inflamed. The causes of the disease, its symptoms, the mechanism of development of the pathological process and the principles of treatment in an adult and in a baby are almost the same. But statistics show that the children's body is affected by eustachitis much more often. This is due to the peculiarities of the anatomy of different ages. The auditory tube in adults is longer and more curved, which makes it difficult for infection to penetrate into it. In this regard, children are much more vulnerable to the disease.
The Eustachian tube acts as a link between the middle ear and the outside world, creating the pressure in the auricle necessary to distinguish sounds. Due to the presence of a hole in it that extends into the nasopharynx, there is a risk of spreading inflammation localized in the throat, nasal cavity and sinuses to the ears.
The occurrence of eustachitis carries a danger, regardless of the age of the patient. But the appearance of its symptoms in babies is especially alarming. The length of the auditory tube in infants and preschool children is no more than 2 cm, while in adolescence it grows up to 3.5 cm, maintaining the same size in adulthood. Due to this specificity, inflammation of the middle ear in babies progresses much faster.
Causes of the disease
The development of tubo-otitis in a child occurs primarily due to the difference in pressure characteristic of the environment and observed in the middle ear cavity. It is she who provokes a violation of the functioning of the auditory tube of the baby. Its mucous membrane becomes inflamed, and the size of the organ increases, preventing the normal passage of air.
Provoke the pathological process of pathogenic bacteria. Most often, tubootitis is caused by microorganisms of the coccal group (streptococci, pneumococci, staphylococci). In most cases, inflammation of the middle ear becomes the result of pathologies that develop in the ENT organs. Initially settling in them, over time, the infection passes to the mucous membrane of the auditory tube.
The causes of the disease can also be physiological in nature. It can develop if the child clears his nose too often (blows his nose) or his sinuses are not properly washed.
The origins of eustachitis in a baby often lie in
- angina;
- flu
- bacterial pharyngitis;
- chronic tonsillitis;
- acute rhinitis;
- diphtheria;
- sinusitis;
- vasomotor rhinitis.
Sometimes salpingo-otitis in infants is the result of allergic manifestations.
Strong changes in atmospheric pressure are capable of provoking the disease (during flights, scuba diving, climbing to high altitudes).
Significantly complicates the course of inflammation in a baby, the presence of:
- cyst;
- polyps;
- curvature of the nasal septum;
- hypertrophy of nasal conchas;
- nasopharyngeal tumors.
Types of pathology
The purpose of the correct treatment of salpingo-otitis in babies depends on the type of disease. By the nature of the course of the disease, they distinguish:
- Acute tubo-otitis. It is a complicated consequence of inflammatory processes that occur in the respiratory organs (influenza, SARS).
- Chronic tubootitis. Occurs due to incorrect therapeutic measures applied at the first stage of the disease.
Inflammation in a child can be observed in one ear (unilateral eustachitis, localized on the right or left) or, in more severe cases, affect both auditory tubes (bilateral salpingo-otitis).
By the nature of the inflammatory process, the following types of tubo-otitis are classified:
- catarrhal. Its development occurs after a viral respiratory disease. It is characterized by a decrease in pressure in the tympanic cavity, which leads to suction of the secret produced in the nasopharynx. As a result, a fluid that does not have an inflammatory nature is released from the ear.
- Serous (exudative). It is a consequence of the course of the catarrhal form of the disease. Due to dysfunction of the Eustachian tube, inflammatory fluid (exudate) enters the tympanic cavity.
- Purulent. Its causative agents are pathogenic bacteria. It is characterized by purulent compartments. As the disease progresses, the inflammation spreads to other parts of the ear.
Signs of tubootitis
The course of otitis media is accompanied by similar symptoms in all age groups of patients, the clinical nature of which is determined by the form of the disease. It can be assumed that the baby has acute eustachitis if the baby has:
- hearing is reduced;
- there is noise or crackling in the ears;
- fluid appears in the ear, overflowing during head movements (turns);
- autophony develops (the baby's voice is heard in his ears);
- the incidence of otitis media is increasing;
- swollen ear canal.
Bilateral tubo-otitis is often diagnosed in young children. Sometimes the disease is manifested by bubble-like rashes on the outer part of the auricle. A typical symptom of this form of the disease is that swallowing, sneezing or yawning bring significant relief to the baby.
For chronic inflammation of the middle ear:
- sudden changes in pressure provoke stuffiness in the ears and the appearance of noise in them;
- hearing loss is observed for a long time, which also progresses.
It is difficult to identify the symptoms of tubo-otitis in infants, since they cannot tell about the signs that disturb them. The change in the state of the baby affects his behavior. He begins to react sharply to touches on the ear, even the lightest ones, and loses his appetite. His sleep becomes sensitive and disturbing. The disease is characterized by the absence of temperature, but in infants it can rise to 38˚C, the baby may shiver. As the inflammatory process progresses, painful sensations are added to the symptoms that prevent the child from eating and sleeping. The disease may be accompanied by:
- nasal congestion;
- headaches and dizziness;
- lack of coordination;
- slight discharge from the ear.
If the pathology is not treated in time, the mucous membrane covering the surface of the auditory tube becomes thinner, and the eardrum is deformed.
Diagnosis of the disease
Tubootitis in children is established on the basis of the totality of:
- anamnestic data;
- clinical manifestations of the disease;
- otoscopy materials;
- analysis of the function of the Eustachian tube.
An important component of the diagnosis is the definition of the type of disease. To identify its nature - infectious or allergic - swabs are taken from the baby's nose. Treatment of tubootitis caused by an infection proceeds much faster.
Drug therapy for tubo-otitis
Due to the severity and complexity of the course of the disease, if a child has signs of it, it is by no means recommended to self-medicate. To prescribe the necessary therapeutic measures, you should contact an otolaryngologist. Treatment should take place strictly under the supervision of a specialist, without deviations from the scheme planned by him. To alleviate the manifestations of the disease, you first need to eliminate the phenomena that interfere with the patency of the auditory tube.
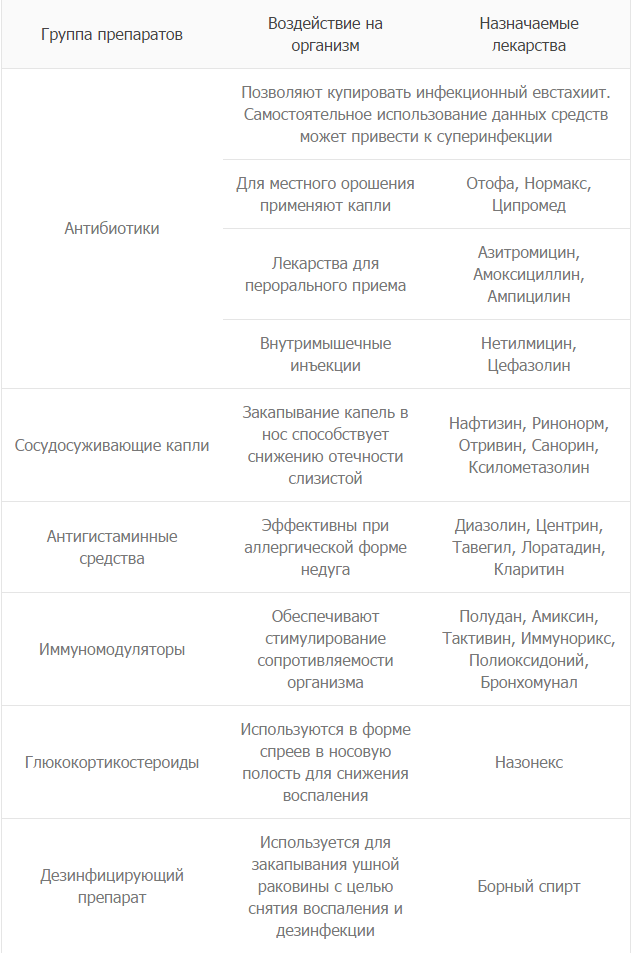
If the inflammation is caused by an infection, medications are usually prescribed:
- Antibiotics. They buy the infection. For local exposure, Otofa and Tsipromed preparations are instilled, Azithromycin, Amoxicillin are used in the form of tablets, and Netilmicin and Cefazolin are used for injections.
- Vasoconstrictor drops. Helps relieve swelling of the middle ear mucosa. Apply nasally. It can be Naphthyzin, Otrivin, Xylometazoline.
- Antihistamines. Used for allergic tubo-otitis. Claritin, Tavegil, Erius, Diazolin have proven themselves well.
- Immunomodulating agents a. Increase the body's natural resistance to infections. Amiksin, Immunoriks, Bronchomunal received special distribution.
- Glucocorticosteroids. Reduce inflammation. They are used in the form of sprays for nasal irrigation. The most commonly used is Nasonex.
- Disinfectants. Remove inflammation and disinfect. They are buried in the ear. Boric alcohol is usually used for this purpose.
If the baby has a fever during illness, you need to give him an antipyretic based on paracetamol.
Physiotherapy activities
To prevent the spread of infection from the nasopharynx to the middle ear, the baby is taught nasal hygiene. Proper blowing your nose is one of the main measures to prevent inflammation of the Eustachian tube. The doctor may prescribe blowing of the auditory tubes. Effective treatment of tubo-otitis involves complexity, a combination of the use of medications with physiotherapeutic measures:
- Pneumomassage of the tympanic membrane. As a result of the procedure, the membrane becomes more elastic, tension decreases and the mobility of the auditory ossicles in the middle ear returns to normal. The risk of scarring of the mucosa, which can lead to hearing impairment of the baby, is reduced.
- ultraviolet irradiation. It relieves pain and acts as an immune stimulant.
- laser therapy. Helps reduce swelling and inflammation, prevents the development of allergies and intoxication.
- UHF treatment. Improves blood circulation, lymph flow, metabolic processes, accelerating recovery.
In most cases, hospitalization for pathology is not indicated. Tubootitis therapy in a hospital setting can be prescribed for newborns and those babies in whom the disease is severe.
Timely initiated therapeutic measures can eliminate tubo-otitis in crumbs in just a few days. If the disease is chronic, then for its treatment it is important to remove the foci of infection. They are various pathologies of the structure of the nasopharynx, provoking an exacerbation of the disease and its transition to a bilateral form. The specialist may advise:
- removal of adenoids and neoplasms;
- tonsillectomy;
- septoplasty.
Disease prevention
Significantly reduce the likelihood of developing inflammation of the middle ear in a child will help the observance of simple rules:
- continue to breastfeed your baby until 1 year old;
- in the process of feeding, keep the body of the crumbs in a semi-vertical state so that the liquid does not enter the ear canal;
- with nasal congestion in a baby, use an aspirator to remove fluid;
- do not start inflammation of the adenoids;
- treat the baby with antibiotics as rarely as possible and do not prescribe them yourself;
- carry out hardening of the baby to strengthen his immunity;
- avoid situations in which sudden pressure drops are possible;
- to prevent hypothermia and finding the baby in a draft;
- minimize the risk of ear injury;
- time to treat colds.
Tubootitis is easily treatable, but neglected inflammation can go into a chronic stage, which is much more difficult to cure, and lead to severe and sometimes irreparable consequences for the baby's hearing. When the first signs of the disease occur, you should immediately seek professional help.